Who can benefit from the Obagi Foaming Gel cleanser?
Anyone who would love to have a professional strength cleanser for deep cleansing feel for their skin
It goes very well with the Obagi Nuderm system which embraces the idea that beautiful skin is healthy skin.
People with normal to oily skin would benefit from the use of Foaming Gel.
Acne prone skin would also benefit as well – especially with the Alfalfa and Borage extracts.
This is a relatively strong cleanser but it is not excessively drying and potentially damaging as bar-soap.
Alternatives to the Obagi Foaming Gel?
If your skin is dry, a gentler cleanser is available from the Obagi Nuderm line called the “Gentle Cleanser.” We also carry the Obagi 360 cleanser which has beads, and also the Clenziderm cleanser which is geared even more for acne skin.
There is a travel size available of the Foaming Gel which is 2 oz in size.
Gentle Cleanser Nu-derm.
Obagi 360 Cleanser.
Clenziderm Daily Care Foaming Cleanser.
Travel sized version is available as well.
Side effects of Obagi Nu-derm Foaming Gel Cleanser
Minimal side effects.
Could be drying in the winter time for some skin types.
Could be drying for dryer skin types.
How to use?
Moisten finger tips and apply small amount to face and neck. Rinse thoroughly.
Can be used with the clarisonic brush.
The cap screws off the bottle and screws back on with a secure locked in feel. There is a small opening on top of the bottle which allows the product to come out the bottle is squeezed lightly.
List price for Obagi Foaming Gel Cleanser from the NuDerm Sytem:
$42.50 – the price can change, and this is the price in 2016
Surgical Artistry is Dr. Tammy Wu and Dr. Calvin Lee’s Plastic Surgery and acupuncture practice in Modesto, California. Dr. Wu and Dr. Lee are a husband and wife surgeons who teamed while they were students at Brown University in 1989. Throughout their academic life, they had been fortunate to have acceptances to wonderful institutions such as Stanford and Harvard.
Dr. Tammy Wu, Modesto Plastic Surgeon had experience using the Keller Funnel many years ago. It adds a bit extra to the cost of the Breast Augmentation procedure and she had decided to purchase various different Keller Funnels to use for her breast augmentation surgeries. She recently talked with the company and is interested in considering the use of the Keller Funnel for all Breast Augmentation cases. Stay tuned for more details on Dr. Tammy Wu’s thoughts on how the Keller Funnel has helped with the breast augmentation surgery itself, and how it helps the patients and perhaps outcomes with the breast implant – in terms of lowering the risk of breast implant capsular contraction, infection, operative time, etc.
Last month, the FDA approved the Natrelle Inspira Breast implant. Dr. Tammy Wu and Dr. Calvin Lee had a chance to be one of the first to see this breast implant at the Plastic Surgery Meeting in Los Angeles last month. This new breast implant combines a high gel fill ratio with the highly cohesive gel seen before in a different breast implant introduced earlier known as the style 410 breast implant. These are also commonly referred to as “gummy” implants.
Dr. Tammy Wu, Modesto Plastic Surgeon, has access to these breast implants if suitable and requested by patients.
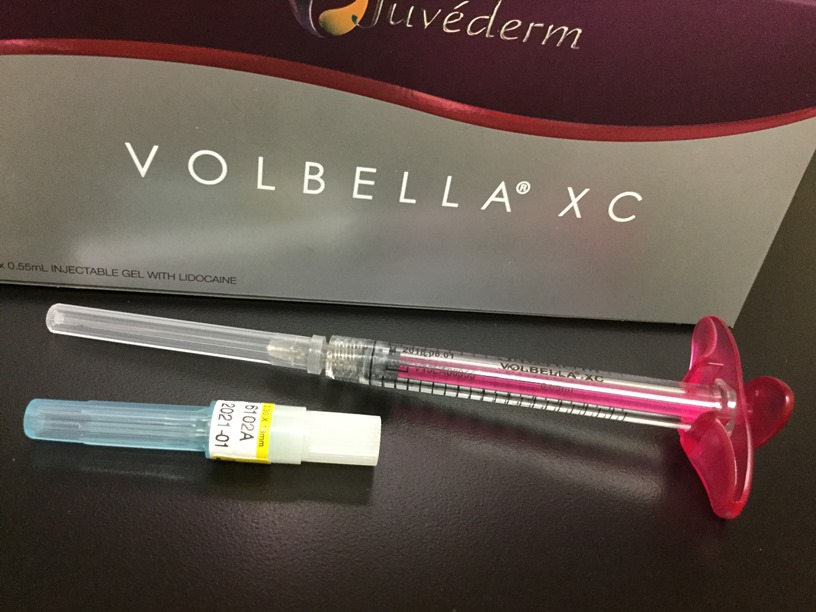
Volbella is a new filler for the Juvederm family of dermal fillers.
I just had a chance to use it for the first time today. I had chosen to use it off label for tear trough correction. In the picture below, I had chosen to attach the Volbella syringe to a 1.5 inch dermal cannula. Soon I plan to try it for the lines around the lips. Sometimes those lines are called the lipstick lines and recently I heard them called “barcodes.”
I wrote this to one of our Surgical Artistry team members on the topic of how to get surgeon-steady hands. It can be practiced and it can be improved upon, much like playing the violin or piano.
“Then you have to think about points of stabilization for the knuckles, wrists, elbows, and shoulders. These points of stabilization need to find possible anchors. For knuckles and wrist – you want to see if you can put parts of the hand on the patient, if not, then put your left hand on the patient and your right hand on top of your left hand this creates an anchor. Then the elbows you have to either anchor it on stable furniture without contamination, or your own body. The shoulders should be loose and flexible and not held stiffly – that will lead to future back problems which will not help with steadiness. It all starts with these thought process of thinking of stabilization points which need to find anchor points and matching them together. I use these concepts all the time when injecting Botox, Kybella and fillers – Voluma, Juvederm, etc. Thus when the patient breathes or moves, my hand moves with the patient synchronously due to anchor points tied to the patient’s head.”
Someone just recently asked me this question and I thought I’d share the answer here.
Dr Lee, what is your filler of choice for this tear trough area under the eyes?
I’ll answer this question as if you were asking me as another colleague injector. Most of the time my favorite tear trough filler is either Restylane-L used straight out of the box or a diluted version of it with about .1-.2 cc’s of either lidocaine or saline. I’m most interested in a new Juvederm offering which is not available to the public yet. Belotero was my previous favorite before Restylane-L, but it was on the too soft side and too short of a duration in my own preference. Before that I used Juvederm ultra for under the eyes, and funny thing, before that I used Restylane-L (what was just called Restylane at the time). Now I’m back full circle to Restylane-L – the old favorite. A blended version of Voluma has also worked very well for the area. But the key is a smooth continuous application placed possibly in two layers is my latest technique. Some tear troughs are so deep that two separate layers of fillers is needed separated by the patients own tissue – this is like making a filler “sandwich”. I hope this sheds some light into what I like. but just about any filler could work in this area, but adjustments need to be made due to swelling and clumping characteristics. In the end, I think it’s more the injector’s technique that matters than the actual product. But if I was teaching a beginner injector, I would probably say a product like Restylane SILK or Belotero – great choices to start with because they are very forgiving!! Forgiving is good in this area, especially if the depth chosen isn’t ideal. However “forgiving” products (belotero and restylane-silk) are usually made up of smaller Hyaluronic Acid (HA) molecules and thus don’t tend to last as long as something with larger HA molecules such as Restylane-L/Juvederm/Voluma.
One more aspect to consider is experience with the swelling characteristics of the HA filler chosen. Restylane-Silk, Juvederm Ultra XC, and Juvederm Ultra Plus XC tend to swell more than Belotero, Restylane-L, and Voluma. I have not personally tried Restylane-Lyft yet under the eyes, but I don’t see a reason for me to try unless a patient was strange and wanted me to do that. There are just so many good choices out there for me already. But stay tuned for the new Allergan product coming out in about 1 month. I think it might be a winner in this department as well.
Answers to questions like this tend to be very complicated when we try to break it down to why we choose what we choose. There are factors regarding skin thickness and color that need to be taken into account regarding if I blend a product or dilute a product too.. And there are choices regarding the tools that we want to use – either a straight needle or various different cannulas.
I’ve had many people ask, but I never got around answering this question. But my favorite filler changes from day to day… so today it’s Restylane-L for tear troughs. It is versatile enough to adjust to most skin conditions especially with dilutional methods, and it fits nicely through a 27 gauge 1.5 inch cannula, and it lasts in this area around 7 months to 1.5 years, and it has built in lidocaine for patient comfort, and it has minimal swelling characteristics to deal with after implantation. Fillers choice is highly personal, just like violin choice is for the violinist.
I was supposed to give a graduation speech in Sacramento for a K-12 school. But instead the date of the graduation got moved earlier, and thus I got the speech out of the way. I had left the day blocked off from patients (from our plastic surgery / acupuncture practice: Surgical Artistry) since it was an opportunity for a day off. I decided to see a dentist. Long story short, I needed a tooth extraction. Tooth got pulled out – Yikes. Funny how things like this happen when you least expect it or when you least want it to happen.
I have a degree in Neuroscience and have done research in physiology and cell biology. I am a board certified General Surgeon and I worked as a trauma surgeon. I am currently an acupuncturist and cosmetic physician specializing in Botox, Juvederm, and Kybella injections. The world of applied exercise physiology is vast and I present some of my opinions. In general, even for the experts, much of how all this comes together is still a mystery. These are just my thoughts, none of this is specific medical advice, and in the end, I’m a back of the pack runner who likes exercise physiology.
First what is conversational pace running?
It’s a running pace where one could hold a conversation while running. One could have gradations in conversational pace: such as slightly difficult conversation pace or super easy conversational pace. So it’s a range of running speed where one’s not gulping for air between each word; phrases of words should come out understandably.
How about heart rate monitoring – how does that compare to conversational pace running.
Some of us just don’t talk while running. Thus we have another way to measure this “conversational pace” by using heart rate monitoring. I like heart rate monitoring because I think it’s more objective. But heart rate varies from day to day, from time of day, and from what we did the day before, etc. So it’s not perfect either.
60-80% of maximum heart rate is conversational pace. Garmin watches will present this as Zone 2 and Zone 3. I estimate my own personal maximum heart rate based on recent experience and for me conversational pace running will fall between 110 and 150 bpm (beats per minute).
Wait, what’s the difference between pace and speed.
They are both a description of how fast we are running. Pace is measured in how many minutes we would finish a mile. Speed is usually miles per hour (mph – in the USA anyway). Most runners use pace, but if you are a treadmill runner – you might like speed measurements because that number you adjust is measured in miles per hour (mph). Basically just talking about the same thing but using different units.
The running world is ruled by those who like using pace. But some of us (like me) like using miles per hour. I made this conversion chart for mph to pace.
What’s the difference between easy miles, conversational miles, and building aerobic base?
Basically same thing in my simple mind.
Why should we spend dedicated period of time devoted to conversational pace running? Can’t we just run at varying speeds and some of it just turns out to be conversational pace?
A time frame of several weeks to several months, depending on your coach, should be spent on building a base of conversational pace running. This base building period could have other types of running, but I believe that each workout should have a focus on a desired outcome. And that each time frame – period of time – should have a predominant focus. We just have one body and it will adapt to most things we throw at it, but if we were to focus what we throw at it, it can grow more strategically.
Some coaches call this periodization – spending several months on a particular goal, then moving on to a different one afterwards, and so on. For example one could work on conversational pace base building for 3 months, then move on to strength training, then move on to speed training with added plyometrics for a few months, etc. It’s not to say that we only do one type of exercise for a period of months, but we should have a predominant type of exercise in the mix.
Thus, I prefer to call a period of conversational pace running – building aerobic base. I’m using aerobic to mean the utilization of oxygen by the muscles. If we run too fast we don’t have enough oxygen for the muscles to use and thus energy has to be made through alternative pathways which we call anaerobic metabolism. There is no “storing” of oxygen in the muscles – it uses what it can extract from the blood stream which flows by. The amount of oxygen presented is influenced by 1. cardiac output, 2. blood surface area (capillaries, etc), 3. amount of oxygen in the blood itself – red blood cells and the oxygen carrying capacity of hemoglobin.
What benefits do we get from spend time in conversational pace running?
I’ve come up with a list of things that improve after a series of conversational paced runs. And much this is more of an improvement than with faster running.
Our bodies become more efficient at burning fat.
Our mitochondria grows larger – mitochondria are organelles within cells. We are particularly interested in our muscle cells. Mitochondria converts fat and glycogen into energy units called ATP. Skeletal muscle cells themselves cannot divide, but they can lay down more protein, get larger, change proportion from fast twitch to slow twitch and grow more mitochondria.
We grow more mitochondria! (so they become larger and more numerous)
Lactic acid does accumulate during purely aerobic exercise – this is why we can go long distances at conversational pace. Lactic acid is something that slows us down and gives us that burning feeling in muscles when we run at faster speeds. Lactic acid is a byproduct of anaerobic metabolism, not aerobic metabolism. Anaerobic means without oxygen.
We use both Fat and Glycogen (stored carbohydrates) at conversational pace running. As opposed to faster running which just uses glycogen.
The slower one goes, the higher proportion of fat is burned relative to glycogen burned. And with the slower speed, we can go longer distances. Thus if we have the time, effectively we’ll burn more calories from fat.
The slower running allows our bones and ligaments to strengthen. To me this is building our base of defense against injury.
Our nervous system starts to develop that “muscle memory” for steady easy runs, and that contributes to running economy – the efficiency of running.
Our lungs and muscles develop a richer, fuller network of capillaries which can extract oxygen. This will lead to a higher VO2(max) – which is a good measure of athletic ability.
Because we can run for longer periods of time at conversational pace, our heart continues adapting by becoming larger and improving our stroke volume. These are also factors contributing to a higher VO2(max).
Why do conversational pace running?
The Kenyans do it.
We become more efficient fat burning machines.
We get bigger and more mitochondria.
We can train longer. And longer training means bigger and more mitochondria.
Injury prevention: Our joints, ligaments, and bones will thank us.
Nerve training: we develop more relaxed running.
More capillaries for the lungs and muscles.
Improved cardiac output.
Improved VO2 (max).
What about running faster than conversational pace?
To be a complete runner, we should do that too. There is a time for that, but it’s probably best after building up a few months of conversational paced running (building aerobic base). Good things come to those who wait. The better our aerobic base, the better our tools for building our anaerobic ability – which includes to moving out the lactate threshold. With the right tools, we’ll more efficiently tackle the lactate threshold challenges in the future. But with those reasons above, we will automatically be faster in distances from 1 mile and above.
But with all these advantages, I conclude for myself that the majority of my running should fall into conversational pace rather than killer mode training.
We will get faster automatically by investing in conversational pace running
In the end most of our runs will probably be conversational paced or upper end conversational paced, otherwise we’ll burn out of our enjoyment for running.
Conversational pace running will automatically give us speed which comes from a better army of mitochondria, higher VO2 (max) (from better heart pump, better oxygen extraction from the lungs from the more numerous lung capillaries, and better oxygen delivery from the more numerous muscle capillaries), better running economy, and my favorite reason: better bones, ligaments and joints to withstand the next set of challenges which may involve actually running faster with interval training. One of the most important things for improving our running is to avoid injury.
I was recently asked via email to answer some questions regarding obesity for a student’s research paper. Here are some of my answers which I thought I would share. These questions are great and I hope I did them some justice.
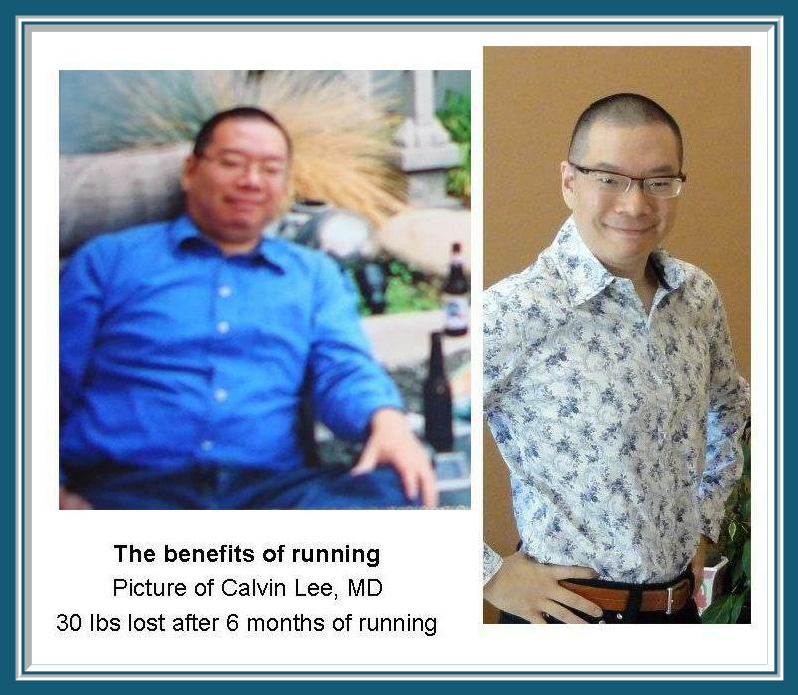
Obesity is a struggle most of us have to deal with. Here’s a picture of me in my attempt to lose weight:
The Obesity Questions
What inspired you to do more with the community outside of your field of practice?
I think I make some decisions which may seem strange, but I like to believe that they are well thought out. I’m originally from New York. In high school, I got accepted to many great universities including Brown University, Harvard, Stanford., etc. I chose to go to Brown for their wonderful program in medicine. I met my wife, Plastic Surgeon Dr. Tammy Wu, at Brown University. She subsequently graduated as the top female student in the medical school program. We started to come to the conclusion that education is what you make of it for yourself, and that applies to where you live. Your community is what you make of it, and we have the responsibility to create and sustain our own environment. A few years after college when I was in my 20’s, I was running a marathon in California and it was during a hypoxic moment during that marathon that I decided that I was going to move to California. Thus I applied for surgery jobs in California. I had then received job offers in San Diego, Orange County, Los Angeles – but turned all those down – and decided on taking a trauma and general surgery position in Modesto, California. Here’s a link to that medical group which I joined in Modesto. A few years later I decided to become an acupuncturist, and while on that journey, I met a few folks in Modesto who had the dream of starting a Marathon in Modesto. I remembered that it was marathon running which brought me to California in the first place. I had often thought that it would be nice to have a marathon in Modesto. At that time I joined my wife’s practice and we named our joined practice, Surgical Artistry. Through Surgical Artistry, we were able to support the creation of a new marathon in Modesto – it was dubbed the Surgical Artistry Modesto Marathon. I have since also become a cosmetic physician with injections of Botox and Fillers. I joke that half of my practice is acupuncture, and the other half is Botox, and then yet another half is surgeries. I am also involved in the classical music world in Modesto. We were founders of the Gallo Center of the Arts in Modesto and supporters of the Modesto Symphony. In summary, we believe that our community is what we make of it, and it requires effort – just like my initial belief about taking responsibility for my own education. While I was working as a trauma surgeon, I’ve come to realize some of the gang related problems with our town, and I was really seeing the worst part of Modesto. I think that has really motivated me to do the opposite and try to focus on the positive aspects.
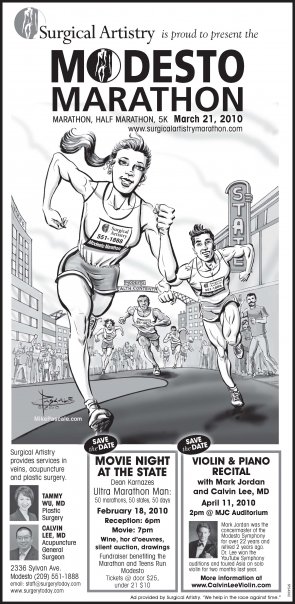
The first newspaper advertisement for the Surgical Artistry Modesto Marathon back in 2009.
2. Why do you think it is important for every community to try and live a healthy lifestyle?
Health is a basic foundation of our lives. And our lives make up the community. Thus if we have personal health, then we can focus on making the rest of the community a better place. That is true for our own families as a microcosmic example. I think we can live by example, and then spread health to others, but it really starts with ourselves. And the community itself is a vibrant organism which needs health as well. So it’s my belief that health leads to a kinder and more compassionate community. Also, if health was a currency – it would be so much more valuable than money.
3. What suggestions do you have for motivating families to become more physically active?
As a doctor, I learn from my patients. I had a particular patient who has been running for most of his life. I asked him how he did that. He said that he saw running as part of his job, and that his job wasn’t done until he got his running done. I have many patients who are so dedicated to their jobs that they feel that they don’t have time for exercise. Thus, I try to tell them to consider exercise – such as walking outside – as part of their job.
I am now in a cosmetic surgery environment, and many of my patients are conscious of their youth. They come to me for Botox and other facial injectable procedures. I tell the patients that exercise is one of the ways to bathe the body in repair mechanisms and growth mechanisms to keep our entire bodies young.
The above two paragraphs refer to strategies I have for adults. As for kids, I encourage them to join group activities in school which involve physical activity. I try to help support a group called Teens Run Modesto which allows for kids to run as a group socially – especially before a workout. It also holds them accountable, and they meet other like-minded kids and mentors. It’s an amazing group.
What I’ve observed from the Teens Run Modesto program is that when the kids are active, the parents start to want to participate too. I think some people call this the “Disney Effect.” If the kids do it, then the parents do it too – like visiting Disney World or Disney Land. I recently learned this concept from the founder of a fitness minded group in Modesto.
And hopefully families will think of social activities to do together which involve more physical activities such as hiking or gardening instead of just passively watching movies. It would be great if the kids would take the lead in their families health. It does make quite an impact on the adults.
Although I do support movies as a form of art. I am also passionate about art. I see much of what I do as a surgeon as a form of art as well.
4. According to recent studies, one in every three children are considered to be obese/overweight. Do you think those rates are going to continue to increase over the next few years?
I think they would increase in the next few years. But it’s our job to try to decrease this rate of increase until one day, hopefully, we will decrease our rate of obesity. I’m hoping that with social media, crowd-effect and education that we will once again be closer to our ideal Body Mass Indexes. I am personally vegan, and I hope that there would be more vegans again in the world. Things tend to go in cycles, and perhaps one day vegans will dominate again and hopefully be healthy vegans rather than potato chip and soda type vegans. If we keep ballooning out at this rate, then we will be lost and our general lifespan on earth will surely decrease.
5. If any at all, what recommendations would you make to professionals in health care services and education industries in raising more awareness with obesity?
Health care professionals need to emphasize prevention of disease. Obesity itself is a disease. Health care professionals should consider leading by example, and we should all immerse ourselves with the latest studies on nutrition. I believe that although there are some complexities of how our bodies process foods, and how our bodies hang on to fat – the first law of thermodynamics apply to our bodies: where increasing our calories spent and decreasing our calories eaten will lead to weight loss. Yes, there are other hormonal factors at play, but calories in and calories out are things that we can measure and thus manage more effectively. There are calorie / step counting watches that make calorie expenditure more fun, and if that is what helps, then I support it. One thing we have to do as health care professionals, I think we have to stop caving into consumer demand for a quick fix. We should be slower to offer that pill or that surgery to fix problems, and try to make patients more accountable for their outcomes.
6. What steps have you taken to reach out to the community? Do you think it was successful and how do you think it will be sustained over the next few years?
I’ve helped to create a new marathon for Modesto. I helped to set up training groups for adults and teenagers for this marathon (which includes other distances like a half marathon and a 5K). In combination with eating more of a vegan diet, I believe that running is one of the most efficient and effective methods of losing weight. I’ve joined in with my local vegan group. And I participate sometimes in our local online facebook pages regarding running and eating well. I think all these efforts have been somewhat successful. We haven’t exactly come up with ways to quantify the differences that we’ve made in this community. But I can say that I definitely, without a doubt, see a lot more runners in our parks in Modesto. It’s like an army of runners. I am now branching out into nearby towns such as Ripon and Manteca for training groups and running events. I just recently started financially supporting (via sponsorship) a group known as Modesto Moves and it just started last Saturday and has about 240 members – walkers and runners.
7. Final question. Do you think it is more important to educate children or adults when talking about obesity and its effects?
Great question. I think if I had to pick one. I would say, educate the children. They are the future, and children have a way of educating adults in a positive manner. As for the other way around. I don’t think kids listen to their parents when they say “Eat your broccoli.” Educating kids is also educating them at a point where they can prevent obesity and its associated diseases. So like any disease – it’s good to catch them early or before it even begins. Thus we should educate the young and focus our energy there.
Dr. Tammy Wu and myself on the cover of the March 2016 issue of Modesto View Magazine. We’re trying to make a difference. Thank you Modesto View for this rare opportunity.
Tummy tuck is not a solution for obesity.
For more information on Tummy Tucks, visit my Tummy Tuck Today webpage: